

ILLUSTRATION: PAPERLILY STUDIO
Legitimately Ill
Sara Gingold
It’s rare to be able to point to a single moment, but I can. I know precisely when I crossed the boundary that separates ‘before’ and ‘after.’
It was 2012. Phnom Penh, Cambodia.
My friend’s apartment was tiny and windowless, with air from the open door barely denting the suffocating heat. We were eating lunch on a fluorescent pink, plastic mat.
It came on suddenly. A fiery heat travelled down my intestines as a wave of nausea made its way up to my throat. I’ll spare you the details of what happened next. Suffice to say that the good news was there was a nearby toilet. But the bad news was that it was a squat toilet, and after six months in South-East Asia, I was only partially acquainted.
For the next two weeks, I was acutely ill with a virus that never got a name.
Months later, I was diagnosed with a chronic illness with the most deficient name imaginable.
——
Myalgic encephalomyelitis (ME) is a disabling and complex disease, with a name that gets stuck on the tongue. So instead, it is commonly referred to by its other name. The one that patients hate, but at least they can pronounce— chronic fatigue syndrome.
The history of the name chronicles the ongoing struggle between the patient and medical communities. It is the tension between the people who live with an illness, and the ones with the power to define it.
In the 19th century, psychiatrist George Beard coined the term ‘neurasthenia’, to describe an illness characterised by physical and mental fatigue, muscle weakness, depression, irritability, lack of concentration and insomnia. Beard believed it was a disease of the nervous system brought on by the stresses of modern life.
Throughout the 20th century, there were various outbreaks of unknown illnesses with similar symptom sets. After an epidemic at the Royal Free Hospital in London in the 1950s, the illness was labelled ‘benign myalgic encephalomyelitis,’ because patients showed signs of inflammation of the brain and spinal cord. The prefix ‘benign’ was later dropped, as unsurprisingly, people didn’t feel it correlated with their lived experience.
Two psychiatrists in 1970 suggested the name ‘myalgia nervosa’, as they believed the illness was caused by mass hysteria. They reached this conclusion, in part, due to its higher prevalence amongst females.
In 1987, after outbreaks in Nevada and New York, the Centers for Disease Control and Prevention (CDC) convened a working group to investigate the condition. The group acknowledged that the name myalgic encephalomyelitis wasn’t broadly accepted. They suggested ‘chronic fatigue syndrome’, which they considered ‘neutral and inclusive.’
There was just one tiny problem— patients hated it.
It’s not hard to figure out why. Chronic fatigue syndrome doesn’t sound like a disabling and complex disease. It sounds like the diagnosis of a perpetual grumbler, somebody who probably needs to have a strong coffee and toughen up. It’s a short journey from ‘chronic fatigue syndrome’ to the more derogatory ‘yuppie flu.’
These days, researchers and patients tend to use the acronym ‘ME/CFS.’ It’s a compromise between the name people can say, and the one those affected can stand.
——
‘You should go home,’ the nurse whispered, as I lay curled in a ball at the Phnom Penh International Hospital.
In the weeks after the onset of illness, my symptoms had changed, but sickness remained an unrelenting feature of life. My quest for answers had reached the outer limits of the Cambodian health system including the services only available to those with savings accounts many times larger than the average annual salary. The nurse was right, I had to go home.
I navigated the airport desperate to avoid bending my massive yellow envelope of X-rays from the local hospital. The flight was awful. I felt exhausted down to my bones but couldn’t sleep. I was fixated on the contents of that envelope and how it might rewrite the course of my life.
When the plane landed in Melbourne, I cried.
The doctors didn’t know what was wrong with me. I wondered if I was dying.
——
An estimated 250,000 Australians live with ME/CFS. This equates to 1% of the population. It probably includes somebody you know.
But that statistic is just an educated guess. ME/CFS doesn’t have a known biomarker that shows up in blood tests or scans, nobody even knows what causes it (though there are some solid theories). This makes diagnosis difficult. In the US, people wait an average of 5 years for a diagnosis and 90% of people are estimated to be undiagnosed. How can you count something if the people affected don’t know they have it?
There are a variety of diagnostic criteria clinicians can use, some considered more rigorous than others. The Australian patient advocacy group Emerge, along with the CDC, favour the National Academy of Medicine (NAM) criteria.
{kind=link}
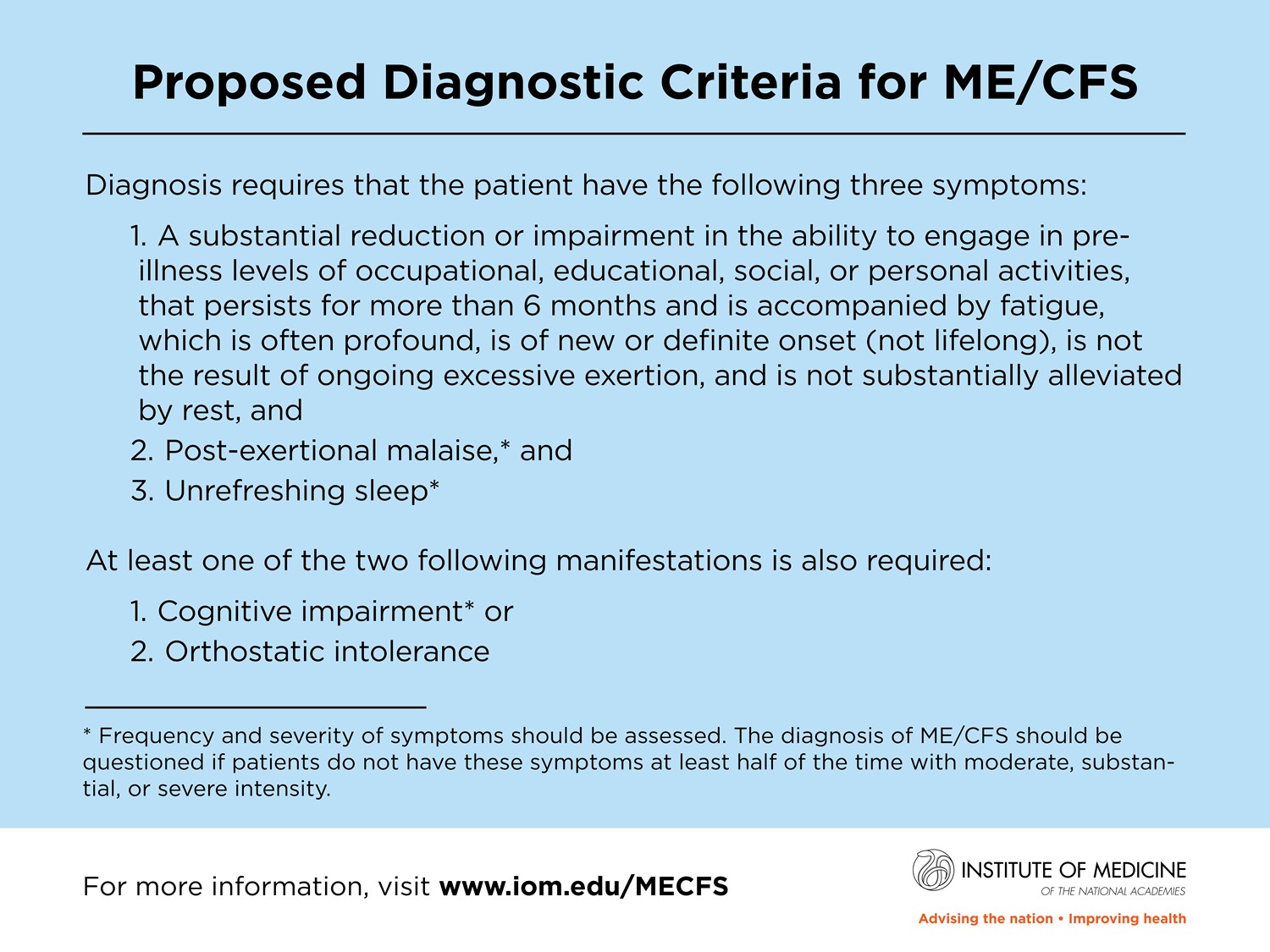
Under the NAM criteria, patients must have:
A substantially reduced ability to do their pre-illness level of activity, accompanied by fatigue, for at least 6 months.
Post-exertional malaise (PEM) - medical jargon for fatigue that gets worse after activity.
Unrefreshing sleep.
And one of the following:
Cognitive impairment.
Orthostatic intolerance - again, medical jargon for symptoms that occur when standing up.
It is also common to experience some combination of muscle pain, joint pain, headaches, light or sound sensitivity, gastrointestinal problems, temperature changes, night sweats, frequent sore throats… the list goes on. For many people, including myself, ME/CFS is triggered by a viral infection. This is why it is not surprising that long-COVID has a similar symptomology to ME/CFS, and some believe that people with long-COVID have ME/CFS.
Symptoms can vary in severity. Approximately 25% of patients are ill enough to be house or bed bound. There are people too sick to eat, to see light, to move, to speak. They lay in the dark all day, the mind a prisoner of the body.
Before ME/CFS, I had not known fatigue. Certainly, I had been tired. But my body had not crashed in on itself after a morsel of activity, protesting by flinging symptom after symptom as it begs for rest. I had never experienced the mental load of calculating the cost of every activity: if I wash the dishes, will I be able to feed the cat? If I vacuum, can I have dinner with my friends?
ME/CFS is an illness that disables a significant proportion of society. So why is it not taken more seriously?
——
If my brain was a hard drive, there would be a folder labelled ‘medical traumas.’
The first file is an appointment not long after I returned to Melbourne. I waited in the specialist’s office, a room that took its brief to ‘stay neutral’ seriously. I made small talk with the medical student trainee, who was reticent, but friendly. Her mouth zipped shut when the specialist walked in.
I don’t know how to tell this story without reducing the specialist to a two-dimensional caricature. In fiction, an antagonist like this would be lazy writing. And she’s a doctor, so she’s probably saved lives. But in my mind, she will always occupy the role of villain. And not just any villain, but the first in a series of villains. The stage-setter.
I tried to tell her about my symptoms. It’s an odd challenge, to describe the sensations of the body in a way that is comprehensible to others. No words fit quite right. It takes you to the borders of the English language and tempts you into the realm of simile in an environment that only tolerates facts.
She let me flounder for a short time, before launching into the cross-examination.
‘Have you broken up with a boyfriend recently?’
‘Did you see a lot of poverty in Cambodia?’
‘Do you have an eating disorder?’
‘Have you ever been sexually assaulted? Raped?’
I started to cry. Less from the contents of the questions and more from the weight of them hitting me one after the other.
She looked at me, all tears and aloneness, and said, ‘It seems to me that you are a very sad person.’
The medical student nodded. 2 against 1. It was final.
Diagnosis: Post-traumatic stress disorder [trauma unspecified at this time]
Treatment: ‘Go out and have some fun.’
——
The term hysteria is derived from the ancient Greek word for womb, hysterika. In ancient Greece, it was believed that an itinerant womb would roam the body in search of its one true desire— sperm. As the womb travelled it would cause all sorts of mischief. A woman’s health issues were nearly always traced back to the thrilling adventures of the wandering womb.
It’s such an odd origin story, that it’s easily dismissed as a quirky fact from a bygone era.
But while the medical community has long accepted that the womb is (perhaps disappointingly) stationary, the echoes of hysteria have rippled through history. Hysteria was not removed from the Diagnostic and Statistical Manual of Mental Disorders (aka the psychological bible) until 1980.
To this day, medical professionals routinely dismiss women’s symptoms or incorrectly attribute them to psychological causes. In 2022, a study found that 71% of all women had been told they had imagined their symptoms. It takes women longer than men to be diagnosed with heart disease and cancer. Medical bias is also an issue for people of colour and LGBTIQA+ individuals, and exacerbated for people with intersectional identities.
In other words: not everyone is considered a reliable narrator of their own experience.
‘Medical gaslighting’ is when a healthcare provider dismisses a patient’s concerns to the point where it is abusive or coercive control.
People with ME/CFS often experience medical gaslighting. ME/CFS is a disease that mostly impacts women (at a rate of 75%) and is of unknown medical origin. Patients effectively have a target on their back from the moment they walk into the doctor’s office.
In a 2019 study, 89.4% of interviewees with ME/CFS said they had experienced dismissive attitudes from health professionals. This included being told ME/CFS is not real, that they were hypochondriacs, depressed, liars, dealing with repressed trauma or just plain lazy.
Honestly, reading that study, the only thing that surprised me was that 10.6% of interviewees hadn’t experienced any medical dismissal. I’d love to meet those people and shake their hands.
——
After six months of illness, an unlikely stroke of luck saw me referred to a specialist who diagnosed me with ME/CFS.
‘I see someone with your symptoms at least once a week,’ he told me. ‘Unfortunately, there’s no treatment I can give you. But I suggest you keep exercising.’
But I couldn’t leave it there. I consulted Dr Google and discovered an exercise physiologist in Melbourne specialising in ME/CFS. Through some deeper online digging, I learned that the program was based on a large UK study, which demonstrated that Graded Exercise Therapy (GET) and Cognitive Behavioural Therapy (CBT) could improve ME/CFS symptoms. Some patients even made a full recovery.
At that moment, I decided I was going to be the clinic’s star patient. I would work hard; I would earn my health back.
A week later, I hauled myself, via two train trips, to an office building in the outskirts of Melbourne. The clinic was up a flight of stairs, which I thought was odd for a place specialising in ME/CFS.
The exercise physiologist was a nondescript blond man in his mid-30s. Through a series of printed diagrams, he explained that the initial virus had deconditioned my body. By gradually increasing the amount I exercised each week, I could return to my pre-illness levels of functioning. Many of his patients had recovered this way, he assured me. It seemed logical.
I followed the program religiously. Every day, I would walk for a set amount of time- regardless of what obstacles my health, or the weather, threw at me. Then each fortnight, I reported my progress to the exercise physiologist.
During one visit, he was sniffling and spurting up phlegmy coughs.
‘No kissing today,’ he croaked. Then after a pause, ‘Well, maybe a little.’
He winked.
I retreated into my chair.
The program’s timeline eventually dictated my walks morph into runs. As I forced myself into a jog, it was like lead was coursing through my veins. I seemed to grow heavier as the meters tracked on, magnet pulled towards the ground.
Later, I would curl into a ball on the couch. My world was barely bigger than the couch in those days. I saw my friends less and I was cutting classes at university.
With each visit to the exercise physiologist’s office, those stairs felt more daunting.
‘You haven’t increased your exercise in ages,’ he said. ‘You won’t get better unless you push yourself.’
I attempted to persevere. Giving up seemed like an abandonment of recovery, and I knew the science was on his side. But I could no longer ignore the fact that my body was rebelling. My days became dominated by a cycle of sleep, vertigo, nausea, and repeat.
‘It feels like I’m getting worse,’ I told him.
‘You are so much better than when you started,’ he said. ‘You’re not remembering correctly.’
But my body just couldn’t go on. I cancelled all future appointments and abandoned most of my exercise. I gave up on recovery and just hoped to return to my pre-exercise program level of sickness.
But I never did.
The guilt nagged at me for years. If I had just stayed in the program, would I have eventually got better?
Was this all my fault?
——
When an illness is viewed as illegitimate, medical gaslighting can occur at a society-wide level.
The study which led me to the exercise program was called the PACE trial. Funded by the UK government, PACE was a large-scale research project led by a group of psychiatrists who hypothesised that ME/CFS was caused by deconditioning following an infection. It tested the efficiency and safety of GET and CBT as treatments and published the results in the Lancet in 2011.
The trial’s outcomes were promising– 60% of people who underwent GET or CBT saw an improvement in their symptoms. And 22% recovered. The science was in: GET and CBT were the way to go.
The PACE trial influenced government policy - the UK’s National Institute for Health and Care Excellence (NICE) guidelines and the US’s CDC both recommended GET and CBT as ME/CFS treatments. Meanwhile, the media lapped up the study, with headlines like this gem from the Independent: ‘Got ME? Just get out and exercise, says scientists.’
But there was something fishy about the PACE trial. It wasn’t obvious to a newly diagnosed me Googling in my bedroom. Remarkably, it wasn’t even obvious to the Lancet’s editors. But many patients believed PACE contradicted the central tenet of their lives— that activity exacerbated symptoms.
But who would believe a group of hysterical patients over a peer-reviewed study published in the world’s most respected medical journal?
In 2015, journalist and public health professor David Tuller published an analysis of the PACE trial which made disturbing revelations about how the study defined recovery.
The PACE team used the self-reporting 36-Item Short Form Health Survey (SF-36) to measure physical function. When the trial began, the researchers decided that if, by the end, a participant had an SF-36 score of 85 (or more) out of 100, they would be considered recovered.
However, mid-way through, they changed the definition of normal functioning to a minimum score of 60. For context, people with congestive heart failure have a mean SF-36 score of 57. Ironically, a person needed a maximum score of 65 to be disabled enough to qualify for the PACE trial. Therefore, it was possible to get worse during the trial and still be considered recovered.
The PACE team also used other criteria to measure fatigue. But they relaxed those benchmarks too.
Tuller’s article also outlined other flaws in the trial. It was overly reliant on subjective self-reporting from patients, rather than objective indicators like how many people returned to work. During the trial, participants were sent a newsletter highlighting the effectiveness of the treatments. The diagnostic criteria for selecting trial participants were broad enough to include people with other explanations for their fatigue. Researchers failed to disclose the conflict of interest arising from their work with insurance companies.
Following a lengthy legal battle, patients were granted access to the raw trial data. Re-analysis against the original benchmarks for recovery found no statistically significant difference between the control groups and people who were treated with GET or CBT.
Following these revelations, 80 prominent researchers signed an open letter to the Lancet editors urging them to pull the paper over ‘major flaws’. In the UK, PACE has been the subject of multiple parliamentary inquiries.
I suspect PACE is the instigator of one of the greatest tragedies of my life. If I had just allowed myself to rest in that first year of illness, would my health have deteriorated so permanently? In that possibility - in the fact I can never know - exists a rage that burns so bright it hurts to look at.
——
Things are changing; long-COVID is re-writing the narrative of ME/CFS. There’s been an influx of research funding and mea culpa news stories. But what’s more encouraging is less quantifiable. The acceptance in the community. The scepticism I don’t see in people’s eyes as I recount my journey from viral illness to significant disability.
Perhaps we’ll get lucky. Maybe this will be the real chasm between ‘before’ and ‘after.’
It will be hard for me to fully trust the medical establishment again. My medical trauma folder is too full, its weight to painful. But I hope to regain my trust in myself. To listen to my body when it tells me I need rest. That I’m sick. That I’m not being hysterical.
Because - to conclude with a sliver of saccharinity - you can’t control whether the world believes you. But you can choose to believe yourself.


Sara Gingold is the Editor-in-Chief at DSC, leading a publication specialising in NDIS news and analysis. In the disability sector, her articles are known for their sharp wit and unflinching analysis. Diagnosed with ME/CFS in 2013, Sara's lived experience of disability shines through in her work. She is currently working on her first novel, a historical fiction account of Florence Nightingale's post-viral disability. She loves animals, books and the disability rights movement.